
NIHR Global Health Research Group on Acquired Brain & Spine Injury
Working to understand brain and spine injury care worldwide, generate and implement innovation, and build capacity in global healthcare workforces.


Scroll
Working to understand brain and spine injury care worldwide, generate and implement innovation, and build capacity in global healthcare workforces.
The NIHR Global Health Research Group on Acquired Brain and Spine Injury (ABSI) unites researchers, clinicians and communities across four continents to transform care for patients with brain and spine injuries in low- and middle-income countries.
Understanding global management approaches and outcomes
Rehabilitation, nursing roles, and identifying deterioration
Randomised trials, algorithms, and novel technologies
Sustainable education and training partnerships in LMICs
Our research is structured around four interconnected themes, each addressing a critical dimension of brain and spine injury care worldwide.

Developing a comprehensive international picture of management approaches and outcomes of brain and spine injury worldwide.
Explore projects →
Developing an understanding of injury rehabilitation, the role of nurses and AHPs in neurosurgical care, and identifying deteriorating patients.
Explore projects →
Conducting randomised trials, developing personalised algorithms and interventions, and evaluating novel technologies to improve patient care.
Explore projects →
Developing capacity through sustainable education and training partnerships and through patient and public involvement in LMIC research activities.
Explore projects →Sixteen projects across four themes spanning 24 countries — from qualitative research and registries to observational studies and randomised trials.
A multi-centre international prospective observational study capturing the global picture of TSI care and outcomes.
Aim: To provide a comprehensive international picture of the management and outcomes of admissions for traumatic spinal injury (TSI) worldwide.
Methods: Multi-centre, international, prospective observational study. Any unit assessing patients with TSI worldwide is eligible. Data collected via a secure online platform in anonymised form, covering demographics, injury mechanism, management, operative details, post-operative care and complications.
Primary Outcome: Frankel grade at discharge or at 30 days following admission, whichever occurs first.
In-depth local epidemiological research at the University Teaching Hospital in Lusaka — Zambia's only spinal trauma unit.
Background: There is one spinal trauma unit in all of Zambia. No epidemiological studies on TSI in Zambia have been published. There is also a social stigma towards patients with spinal injury which limits support, treatment and rehabilitation options.
Work Package 1: Prospective observational data collection on demographics, clinical state, pre-hospital, emergency, intensive care, surgical and rehabilitation care at UTH Lusaka.
Work Package 2: Functional outcome and quality of life assessed at discharge, 3, 6, 12 and 24 months via telephone calls, clinic appointments and home visits.
Impact: Will lead to designated care pathways and infrastructure requirements for sustained improvement in Zambia.
Mapping the virtually unknown burden of brain infections and their neurosurgical consequences across Sub-Saharan Africa.
Background: Brain infection is a typical disease of poverty. Its epidemiology and neurosurgical consequences are virtually unknown, making it impossible to plan appropriate interventions.
Settings: Centres across Sub-Saharan Africa (South Africa, Zimbabwe, Malawi, Kenya, Nigeria, Ghana, Uganda) utilising the CAANS network.
Inclusion: Patients with diagnosed or suspected brain infections (bacterial, tuberculous, parasitic, malarial) with neurosurgical complications including raised ICP, hydrocephalus, brain ischaemia, and mass lesions.
Data collected: Patient demographics, clinical presentation, brain imaging, infectious neurological complications, treatments, clinical outcomes, causes of delay in diagnosis, and microbiological flora.
Assessing care quality and delays for TBI patients transferred to neurosurgical units in Tanzania and Zambia.
Background: Data from LMICs suggests that patients transferred to neurosurgical units from neighbouring hospitals experience much larger delays to receiving care. A key concept is that only part of brain injury occurs at the time of trauma, while the rest evolves over hours and days (secondary injury).
Work Package 1: Prospective inclusion of all TBI patients admitted to neurosurgical units in Dar es Salaam, Tanzania and Lusaka, Zambia over a 1-year period. Mode of transportation, initial management, time to imaging, referral and transfer all evaluated.
Work Package 2: Cross-sectional survey of resources available across first, second and third level hospitals in Tanzania and Zambia.
Work Package 3: Qualitative semi-structured interviews with healthcare staff at a sample of hospitals to understand quality of care and barriers to timely treatment.
A participatory qualitative study examining how nurses and AHPs deliver neurosurgical care for ABSI patients in LMICs.
Background: Nurses and AHPs are internationally recognised as a highly skilled workforce essential to safe, effective patient care. In LMICs they typically work with minimal budgets and limited resources. There is a lack of adequately trained nurses and AHPs in neurotrauma — as the largest component of the healthcare workforce, they are strategically positioned to make a significant contribution to improving outcomes.
Aim: To examine the role of nurses and AHPs in delivering safe, effective and evidence-based neurosurgical care in LMICs.
Methods: Participatory methodology with nurse and AHP collaborators from India, the Philippines and Myanmar as co-investigators. Qualitative study with semi-structured interviews and focus groups. Sample size approximately 20-30 participants, informed by data saturation.
A systematic assessment of rehabilitation provision for ABSI patients across low- and middle-income country settings.
Background: Rehabilitation post-TBI is an effective way of mitigating disability and improving quality of life. However, in LMICs, rehabilitation services are frequently absent, under-resourced or inaccessible. Understanding the current landscape is a prerequisite for developing effective, locally appropriate interventions.
Aim: To describe the availability, accessibility and quality of rehabilitation services for ABSI patients across LMIC settings.
Methods: Mixed methods combining a structured survey of rehabilitation resources with in-depth qualitative interviews with rehabilitation professionals, patients and caregivers across partner sites in Africa and Asia.
Leveraging systems engineering to map and re-architect patient journeys from first presentation through to neurosurgical care in Myanmar.
Background: A systems engineering approach is being used to understand care pathways in LMIC settings, building on qualitative and quantitative network maps of patient flow in neurosurgical hospitals in Myanmar (Yangon General Hospital).
Inpatient component: Using the Yangon Early Warning Score (YEWS). Qualitative data drives a tool design process via a Delphi process with Burmese colleagues, validated against the Glasgow Coma Scale before piloting.
Admission component: Data-driven modelling of patient flow within YGH, combining prospective data collection with GEO-TBI data to build quantitative network maps and inform care re-architecture.
Referral component: Mapping emergency paediatric neurosurgery pathways in Myanmar, with course design, piloting and validation using established educational research methodologies.
Understanding the critical and often unrecognised role of non-healthcare workers in supporting ABSI patients in Uganda.
Background: In many LMIC settings, family members and community caregivers play a central role in the care of patients with brain and spine injury. This role is frequently unrecognised and unsupported, with significant consequences for caregiver wellbeing and patient outcomes.
Aim: To understand pathways of care for patients with brain and spine injury and the role of non-healthcare workers such as family and community members in Uganda.
Methods: Qualitative research in collaboration with partners at Makerere University, Mbarara University, UUKHA, Association of Anaesthesiologists of Uganda, Mulago National Referral Hospital and Mbarara Regional Referral Hospital. Includes workshops with healthcare workers and community engagement via the SafeBoda Academy.
Future work: Recruitment of Ugandan Research Fellows, quantitative data collection, and reciprocal exchange visits to Cambridge.
A randomised trial comparing two hyperosmolar agents for post-traumatic intracranial hypertension in LMIC settings.
Background: Post-traumatic intracranial hypertension is very common and, if not treated promptly, can cause brain ischaemia, stroke and death. Both mannitol and hypertonic saline are widely used, but there is limited high-quality evidence comparing their effectiveness, particularly in LMIC settings where monitoring and intensive care resources are limited.
Aim: To determine which hyperosmolar agent is more effective at reducing intracranial pressure following traumatic brain injury.
Design: Randomised controlled trial. Leverages close links with the NIHR Brain Injury MedTech Co-operative and builds on lessons from the RESCUE-ASDH trial (highest recruiting site: NIMHANS, Bangalore).
A before-after intervention study evaluating antibiotic-impregnated shunts at Tikur Anbessa University Hospital, Addis Ababa.
Background: Shunt infection is a devastating complication of hydrocephalus surgery, with baseline rates of approximately 24% at this site. Antibiotic-impregnated shunts significantly reduce infection in high-income settings (BASICS trial), but have not been evaluated in LMICs where the burden is greatest.
Design: Before-after intervention cohort study: baseline (12 months), intervention rollout (9 months), follow-up (6 months), sustainability (15 months). Target: 645 operations total.
Setting: Tikur Anbessa University Hospital and affiliated hospitals in Addis Ababa. All patients of any age with hydrocephalus requiring a first ventriculoperitoneal shunt.
Primary outcome: Shunt failure due to infection at 6 months after insertion.
Developing and validating a portable AI-powered ophthalmoscope to detect raised intracranial pressure in resource-limited settings.
Background: Papilledema (optic disc swelling due to raised intracranial pressure) requires urgent neurosurgical intervention. Traditional ophthalmoscopy requires training and expensive equipment rarely available in LMICs. AI-enabled smartphone-based fundus photography offers a transformative approach to detecting raised ICP without specialised equipment.
Setting: Primary sites in Tanzania (Muhimbili Orthopaedic Institute) with portable ophthalmoscope equipment provided through NIHR ABSI funding.
Significance: Part of the EyeVu Consortium for global neurosurgery (Lancet Neurology, 2023). Allows wider screening for raised ICP in communities without direct access to ophthalmology clinics or brain imaging.
Evaluating a portable near-infrared spectroscopy device for bedside TBI diagnosis at NIMHANS, Bangalore, India.
Background: Identifying patients with traumatic intracranial haematomas who require urgent surgery is a key challenge in settings where CT scanning is unavailable or delayed. Near-infrared spectroscopy (NIRS) offers a non-invasive, bedside approach to detecting intracranial blood.
Aim: To evaluate the performance of a new portable NIRS device for detection of traumatic intracranial haematoma in a resource-limited setting.
Significance: A validated portable NIRS device could transform triage and surgical decision-making for TBI patients in LMICs where CT scanning is not readily available, particularly in district hospitals and pre-hospital settings.
Validating a step-by-step stratified TBI treatment protocol adaptable to varying resource levels across Colombian hospitals.
Background: Investigators in Cali, Colombia created BOOTStraP (Beyond One Option for Treatment of Traumatic Brain Injury: A Stratified Protocol), which provides step-by-step treatment options spanning low, intermediate and high resource settings, across field transport, emergency department, neurosurgery, and ICU phases.
Aim: Prospective observational study of resources, treatments, mortality and morbidity for severe TBI patients in 4 Colombian hospitals over 27 months, examining adherence to the BOOTStraP protocol and its impact on outcomes.
Impact: If effective, BOOTStraP could provide an inexpensive and rapidly deliverable resource throughout LMICs and underserved areas where expertise and resources are limited.
Developing and validating a text message system for remote assessment of TBI patient outcomes using the Glasgow Outcome Scale Extended.
Background: Long-term outcome data beyond discharge is generally not reliably recorded in LMICs. With over 5.2 billion mobile subscribers globally, SMS technology offers a widely accessible follow-up tool. The Patient Response Interface through SMS (PRISMS) platform delivers text-message surveys based on the gold-standard GOS-E.
Aim: To examine if SMS can be used to follow up TBI patients (via the Telehealth Usability Questionnaire) and to validate GOS-E-SMS against the standard GOS-E.
Design: Service evaluation over 12 months with a preliminary pilot for validation. Convenience sample of 50 patients enrolled at first outpatient clinic visit (typically 1-month post-injury).
Embedding and supporting LMIC-based research fellows with structured research training, BMJ publication support, and PhD opportunities.
Approach: Substantial salary support for local Research Fellows in Ethiopia, India (two institutions), Colombia, Pakistan, South Africa, Brazil, Cameroon, Malaysia, Myanmar, Zambia and the Philippines. Fellows are co-investigators on local projects and receive structured research training.
BMJ Research to Publication: Two years of online access to BMJ Research to Publication resources for all collaborating institutions, to further nurture local research capacity.
PhD opportunities: PhD fees funded for Research Fellows in Zambia (joint UTH/Cambridge supervision), Kenya (joint AKU/Cambridge), and Cambridge public health.
A reciprocal fellowship programme enabling LMIC and HIC researchers to undertake placements and build long-term collaborative relationships.
Background: Fellowship exchange programmes where LMIC researchers have placements in high-income countries and vice-versa enable the development of long-term, sustainable, academic and clinical partnerships that extend beyond the life of the grant.
Programme: Supporting reciprocal exchange visits between the UK and LMICs to strengthen partnerships, deliver crucial research stages, and build lasting relationships. LMIC researchers travel to Cambridge; UK researchers travel to Uganda, Zambia, South Africa, Ethiopia, Pakistan and other partner sites.
Delivering and expanding practical neurotrauma training courses for surgeons, anaesthetists and nurses across LMIC partner sites.
ZAM CAM 2024: The first post-pandemic ZAM CAM Neurotrauma Course was delivered in Lusaka, Zambia (February 2024) by six Cambridge clinicians and researchers. Over 50 healthcare professionals attended — neurosurgeons, general surgeons, orthopaedic surgeons, anaesthetists, nurses and physiotherapists from across Zambia. Sessions covered assessment, pathophysiology, log-roll, cervical collars, burr-holes and spinal instrumentation.
Partnership: The ZAM CAM programme is part of an ongoing Cambridge-UTH Lusaka partnership established in 2017, focusing on education, research and clinical knowledge exchange.
Future plans: Funding secured to develop and deliver two additional hands-on training courses at partner sites, evaluated using established educational research methodologies.
Embedding CEI across ABSI projects and evaluating which models of public involvement are most effective in LMIC neurotrauma research.
Background: A CEI Co-Applicant (Prof. Charlotte Whiffin, University of Derby) was embedded in the team from the outset. We recognise the value of public involvement to the design and conduct of rigorous and relevant research, and the importance of stakeholder engagement in disseminating research to increase its reach and impact.
Aim: To embed CEI into a range of ABSI projects and evaluate which models of public involvement are most effective in LMIC neurotrauma research.
Activities to date: Community advisory boards (Pakistan, Ethiopia); brain awareness campaigns (South Africa, India, Cameroon); CEI Webinar November 2024 (100+ registrants); Uganda Health Data Workshop (January 2024); clinical practice guideline co-design with communities in Colombia.
Our research has appeared in leading international journals including the New England Journal of Medicine, The Lancet Neurology, and BMJ.
"The process of working collaboratively with groups of people who are affiliated by geographic proximity, special interests, or similar situations, with respect to issues affecting their well-being."
That all global neurosurgical research is undertaken in collaboration with the communities who are most likely to be affected by the research outcomes.
To foster inclusive and community-driven ABSI research by establishing collaborative partnerships and facilitating community involvement in all stages of the research process.
60 learners from schools in Khayelitsha joined the African Brain Child Initiative's annual event. Almost 2,000 cases of suspected TBI are seen each year at Red Cross War Memorial Children's Hospital — only 4% of severely injured child car passengers wore seatbelts. The Be Quick to Click campaign was central to this year's event.
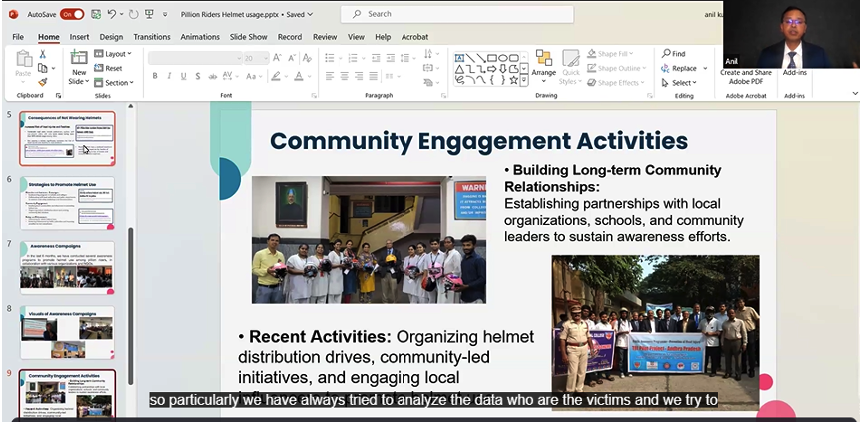
An awareness programme on head injury and pillion rider helmet usage engaged approximately 250 engineering students, covering real-life narratives, the Good Samaritan law, and practical guidance on preventing head injuries.
Ongoing awareness campaigns and lectures on head injury prevention and helmet usage targeting pillion riders — delivered across colleges, communities and societies with Rotary Club participation.
"The Power of Partnership: Strengthening ABSI Research through Community Engagement and Involvement" — Over 100 registered, 55 attended live. Speakers from India, Cameroon, South Africa, Pakistan, Ethiopia and Colombia. 33/34 respondents said they would attend another CEI webinar.
Stories and updates from our researchers working across the globe. Click any post to read in full.



Find ABSI researchers at these upcoming international conferences and meetings.
Society of British Neurological Surgeons Annual Meeting. 12–14 March 2025.
Find out moreEuropean Association of Neurosurgical Societies Congress. 5–9 October 2025.
Find out moreTraining fellowship opportunities in Jamaica and Nepal, supporting the development of global neurosurgery capacity.
Find out moreResearchers, clinicians and collaborators from across the world united by a shared mission.
For all enquiries about the NIHR GHRG ABSI, research partnerships, or opportunities, please reach out to our project manager.
On 26th November 2024 we hosted our first CEI webinar: The Power of Partnership: Strengthening Acquired Brain and Spine Injury Research through Community Engagement and Involvement. This event showcased the excellent work of our partners who are working with communities to drive meaningful, inclusive, and impactful research.
Presentations from Mr Anil Kumar, Dr Franklin Chu Buh and Associate Professor Ursula Rohlwink. Mr Kumar spoke passionately about the critical importance of helmet use for pillion riders and a specific project to increase their use in India. Dr Chu Buh described his pilot project to reduce occupational injury and increase road safety in Cameroon. Associate Professor Rohlwink discussed the African Brain Children Research Initiative and their outreach to inspire the next generation of neuroscientists in South Africa, while increasing understanding of the importance of seatbelt use in children.
This session focused on more formal approaches to engaging communities within the research process. Dr Almas Fasih Khattak reviewed the community advisory board at Northwest General Hospital, Pakistan. Dr Abenezer Tirsit described the CAB at Addis Ababa supporting research on neural tube defects. Nadya Castillo Aragon and Luz Llined Mendoza presented their collaboration with communities to develop clinical practice guidelines for TBI in Colombia.
Over 100 people registered, 55 joined live. Of 34 completed evaluation forms, overall quality was highly rated — 33/34 said they would attend another CEI webinar. Attendees highlighted the importance of advocacy, social media influencers in public health messaging, and practical examples shared by speakers.
"Community engagement is of utmost importance in curbing the incidence of neurological conditions."
"The presenters shared practical examples and case studies that demonstrated the real-world impact of partnerships."
Thank you to all our speakers, Co-Chair Mr Angelos Kolias, Dr Brandon Smith, and everyone from the CEI group who made this event a success.
In January 2024, a research team from ABSI and the International Health Systems Group at the University of Cambridge co-facilitated a community engagement workshop in Kampala, Uganda — a crucial step in our ongoing research on health data management and technology adoption in low-resource settings.
As healthcare becomes increasingly digitised, vast amounts of data are being generated about populations and individuals. This has the potential to revolutionise healthcare technology and medicine, but also raises important questions about data safety, confidentiality, and equitable access.
Our workshop took place at Mulago National Referral Hospital, bringing together 16 participants including medical students, allied health professionals, and specialty doctors. Topics: mobile phone usage and cellular network accessibility across Uganda, and attitudes towards health data storage and sharing.
Phone ownership varies greatly based on geography, socioeconomic status, and age. Many families share a single device or use basic feature phones, and there is frequent SIM card swapping to manage costs. Limited infrastructure for electronic health records exists, with fragmented systems between specialties; patients often carry their own paper medical records.
We are grateful to our academic partners, the Uganda-UK Health Alliance (UUKHA), and all participants. This workshop was supported by the Wellcome Trust and InciSion Uganda. Next steps include collaboratively exploring infrastructure gaps and ensuring our approach addresses data safety and equitable access.
The 77th WHA took place in Geneva at the end of May 2024. The ABSI delegation — Prof Peter Hutchinson, Miss Sara Venturini, Dr Tommi Korhonen, Prof Tariq Khan and Dr Almas Khattak — attended several satellite events advancing global surgical care.
The G4 Alliance is a global coalition working to ensure everyone has access to essential surgical, obstetric, trauma and anaesthesia (SOTA) care. Prof Hutchinson, as SBNS President, represented the Society of British Neurological Surgeons as they joined the G4 Alliance as a member organisation. The G4 Outreach Day covered surgical health system strengthening, referral pathways, surgery in non-communicable disease management, and the role of data in driving advocacy. Tariq Khan and Peter Hutchinson gave a joint presentation on making TBI a notifiable disease and the GEO-TBI registry.
The ABSI team also attended: Revolutionising Global Health — Multisectoral Collaboration on NCDs; Global Surgery Foundation's Women's Health Equity event; Congenital Anomalies and Universal Health; Strengthening Health Systems through Surgery (NIHR); and Data-Driven Transformation: The Operative Encounter Registry.
The ABSI delegation also participated in the annual Walk the Talk event promoting #HealthForAll.
In February 2024, a team of six clinicians and researchers from the University of Cambridge and NIHR ABSI travelled to Lusaka, Zambia to run the ZAM CAM Neurotrauma Course — the first since the COVID pandemic.
The ZAM CAM course is part of an ongoing partnership between the University of Cambridge and University Teaching Hospitals in Lusaka, established in 2017 and supported by the NIHR through the ABSI group, focusing on education, research and clinical knowledge exchange.
The three-day course brought together over 50 healthcare professionals from across Zambia — neurosurgeons, general surgeons, orthopaedic surgeons, anaesthetists, nurses and physiotherapists. A mixture of lectures and practical sessions covered assessment, pathophysiology of brain and spine trauma, log-roll technique, cervical collar application, burr-hole procedures to evacuate intracranial haematomas, and comprehensive spinal procedures including instrumentation.
A great opportunity to connect with colleagues in Lusaka, discuss neurotrauma management in remote parts of Zambia, and create new collaborations. This course is part of a larger body of NIHR ABSI-supported work including academic research projects to map and improve care of patients with acquired brain and spine injuries in Zambia.

My research focus is to understand the pathways of care for patients with brain and spine injury, and the role of non-healthcare workers such as family and community members in care — both in the community and in hospital.
We collaborate with partners including academics at Makerere University, Mbarara University of Science and Technology, the Uganda UK Health Alliance (UUKHA), Association of Anaesthesiologists of Uganda (AAU), Mulago National Referral Hospital and Mbarara Regional Referral Hospital.
In January 2024 I was part of a group of six researchers from the International Health Systems Group travelling to Uganda. We undertook a workshop with healthcare workers in Mbarara RRH — a fantastic opportunity to understand how the healthcare system works for patients with brain and spinal injury. We also learned about a new neurosurgical HDU being established there. The journey from Kampala to Mbarara takes about five hours through rural Uganda, making visible the challenges faced by trauma victims including poor road conditions and long travel times to reach hospital.
Back in Kampala I worked with Henry at UUKHA to meet community representatives to discuss our upcoming research plans and review participant information leaflets. I was given a tour of the SafeBoda Academy, with its focus on education, road safety, helmet provision and high-visibility jackets. These meetings have already led to very positive discussions and formed relationships which we hope to continue throughout the research.